
What is vocal fold paralysis?
Vocal fold paralysis refers to one or both vocal folds being unable to move. This usually results from injury to the laryngeal nerve or nerves.
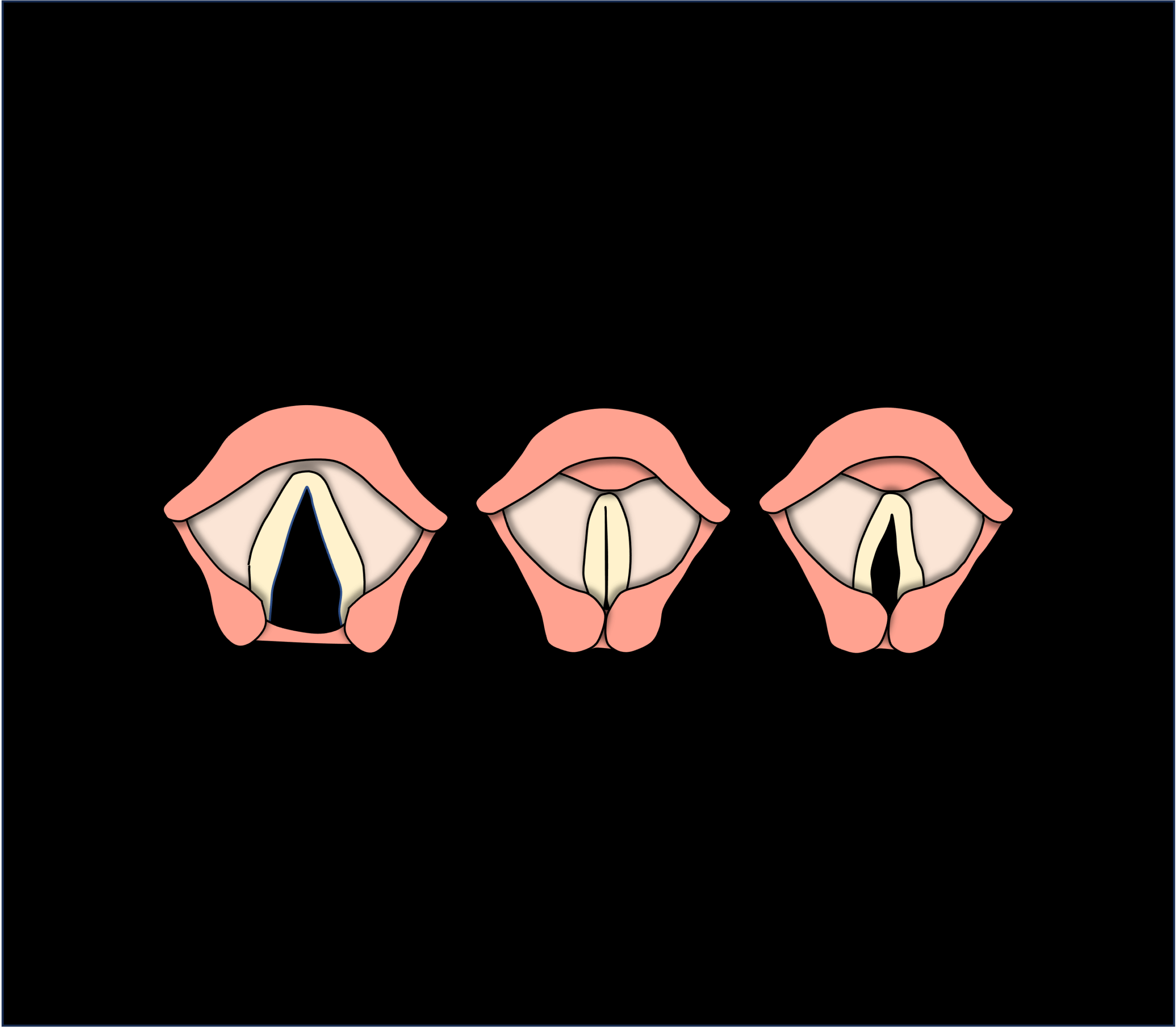
To understand more, we need to know a little bit about how the vocal folds work to produce voice. The vocal folds are two muscular folds with a soft tissue covering. They are located in the voice box just above the windpipe. When we breathe, the vocal folds open in a "V" shape and when we speak they come together and close. When the vocal folds close, air coming up from the lungs enables them to vibrate and produce voice.

The laryngeal nerves control the opening and closing movements of the vocal folds. These nerves follow a complex pathway. They travel from the brain, through the neck into the chest. There they make a U-turn and travel back up to the voice box.
In vocal fold paralysis injury somewhere along the nerve pathway prevents the vocal folds from opening and closing normally.
Next, let’s take a look at some common problems that vocal fold paralysis can cause.
What problems can vocal fold paralysis cause?
Weak voice
Weak voice is the most common symptom of a paralysed vocal fold. This occurs because the vocal folds cannot close properly, resulting in a gap between the vocal folds during voicing. Air leaking through the gap causes the voice to have a weak, breathy quality. Patients may also experience breathlessness on speaking and difficulty straining and lifting heavy objects due to excessive air leakage,
Choking on swallowing
Sometimes swallowing is difficult and choking can occur particularly when drinking liquids. In addition, coughing can be weak or ineffectual and does not seem to clear the throat.
Difficulty breathing
Paralysis of both vocal folds is rare but can cause life-threatening breathing difficulty. This happens because the vocal folds usually become immobilized in the mid-line of the voice box. Hence they cannot open into the normal “V” shape for breathing.
What causes vocal fold paralysis?
There are many possible causes of vocal fold paralysis. All of them in some way cause injury to the nerve supplying the vocal folds.
Certain surgical procedures in the neck and chest can injure the laryngeal nerves. Such procedures include thyroid surgery, neck spine surgery, and sometimes surgery on the heart and lungs. Tumours in the neck, chest, or base of the skull can also cause vocal fold paralysis. Hence it is important to look for the cause carefully. In addition, radiotherapy to the head and neck can occasionally injure the vocal fold nerve. Furthermore, people with neurological conditions such as stroke or Parkinson’s disease can also develop vocal fold paralysis. There are usually other nerve related symptoms in these conditions, and the vocal fold paralysis is part of that condition. Finally, some viral infections can cause vocal paralysis, and a proportion can be idiopathic, meaning there is no identifiable cause.
How do we diagnose vocal fold paralysis?
Confirming the diagnosis
We usually suspect the diagnosis from a change in the patient’s voice. Typically, the voice is weak and breathy. There may have been an event such as surgery, trauma, or an infection that preceded onset of symptoms.
A key part of the examination is diagnostic laryngoscopy. We do this in the outpatient clinic using a small, flexible camera through the nose to visualize the vocal folds. From here, we can tell if the vocal folds are moving. We may use a special strobe light to examine how well the vocal folds vibrate and close. We call this a video-stroboscopic examination.
Identifying the cause of paralysis
We may need to do some tests to look for the cause of paralysis. The first investigation is usually a CT or MRI scan of the neck and upper chest. These scan the nerve pathways to the voice box. Sometimes we need to do a thyroid ultrasound scan, or examine the esophagus using transnasal esophagoscopy. Occasionally we do blood tests to get more information.
Predicting recovery
Knowing what caused the paralysis can help predict if recovery is possible. For example, a stretched or bruised nerve is more likely to recover than a cut nerve or one damaged by tumour.
Laryngeal electromyography is a test that can provide further information about vocal fold function. The test involves passing a very fine needle through the neck into the muscles of the vocal fold. This allows us to measure electrical activity within the muscle. The test can help confirm the diagnosis of vocal fold paralysis if this remains unclear after diagnostic laryngoscopy. Furthermore we can use it to assess the degree of injury and therefore possibility that the vocal fold will recover. This may influence the type to treatment required.
How do we treat one-sided vocal fold paralysis?
Treatment for one and two sided paralysis is different
One-sided vocal fold paralysis is much more common than two-sided paralysis, so let’s look at how we treat this first. I’ll talk more about two-sided paralysis later.
Is doing nothing an option?
Doing nothing is an option particularly if symptoms are mild and we think that the vocal fold could recover.
Symptoms from vocal fold paralysis can be very mild or have significant impact on quality of life. For example, hoarseness not critical to an infrequent voice user could be devastating to someone reliant on voice for livelihood. This may guide the decision on whether to intervene early.
In more severe situations vocal paralysis can even lead to life-threatening chest infection. This happens because the vocal folds cannot close to protect the windpipe when eating and drinking, and coughing is difficult. Intervention is more urgent in this situation.
Speech therapy and voice physiotherapy
Speech therapy and or voice physiotherapy can help patients with milder symptoms strengthen their voice and improve projection. It can also be useful for patients with vocal paralysis who have swallowing difficulty.
I generally do not advocate prolonging speech therapy at the expense of surgical intervention, unless clear improvements occur early. Early surgery can lead to better long-term outcomes even if the nerve does not recover. It prevents muscle misuses developing that can hamper voice improvement with later surgery. However waiting for a few weeks, and occasionally months if there are signs of improvement, is not unreasonable.
Speech therapy can also help after surgery to fine-tune the voice.
Injection medialisation
What is injection medialisation?
Injection medialisation involves injecting a filler material into the paralysed vocal fold to bulk it up. Bulking helps close the gap between the paralysed and normal vocal fold. Hence the voice becomes stronger and swallowing easier.
What do you inject?
The most common material we inject is hyaluronic acid. Although it is possible to inject a variety of materials. Hyaluronic acid is very biocompatible and is commonly used in other parts of the body as a filler. It typically lasts 6 to 12 months, but can last longer.
How do you inject it?
We can inject it under local anesthetic through the neck, or under general anesthetic through the mouth. You can read more about how we reach the vocal folds through the mouth in the post on micro-laryngeal surgery. The video below shows a vocal fold injection under general anesthesia for a paralysed left vocal fold
Advanced ENT Centre
I prefer to do the injection under general anesthesia if we need it to be more precise. However local anesthesia is an option if precision is not critical and the patient prefers. The local anesthesia option is also suitable if the patient is not fit for general anesthesia.
When do you do the injection?
Doing the injection early on can improve quality of life by making the voice stronger and swallowing safer. In addition, an early injection can avoid the need for more invasive procedures later, even if paralysis does not recover. This is particularly so if there is some residual function of the nerve. Hence, we sometimes do an injection medialisation even if we expect the voice to eventually recover.
Medialisation thyroplasty
An alternative to doing the injection is to place an implant into the voice box through a neck incision. We perform this surgery under local anesthetic and sedation. This means that you are asleep for most of the procedure. However we need to wake you up to test your voice when we put in the implant. We usually use implants made from gortex or surgical-grade silastic. Although other options are available. Medialisation thyroplasty improves the voice permanently but is also reversible if necessary.
Other surgical approaches
We sometimes need to consider other variations of surgery. These include adjusting the cartilage at the back of the voice box or re-innervating the voice box. Reinnervation involves connecting a healthy nerve from another muscle to the damaged voice box nerve. The newly-joined nerve takes some months to regain function, and vocal fold movements may not fully return to normal.
The goal of all these procedures is to get the vocal folds to meet in the midline. This enables them to vibrate against each other so that the voice is as strong as possible. As the vocal folds also need to close during swallowing, these surgical procedures can significantly improve swallowing too.
How do we treat bilateral (two-sided) vocal fold paralysis?
With both vocal folds paralysed, breathing becomes the primary concern as the vocal folds typically become immobilised in the midline. Breathing difficulty can range from breathlessness during exertion or exercise, to life-threatening breathlessness even at rest.
Very often patients with severe symptoms will have needed a tracheostomy. This is a breathing tube inserted into the windpipe through an incision in front of the neck. The tracheostomy bypasses the obstruction at the vocal folds. Hence, the patient breathes through the tracheostomy rather than through the nose and mouth.
Having to live with a tracheostomy can be devastating for patients. However we can overcome the need for the tracheostomy by creating a surgical opening between the vocal folds. This operation uses micro-laryngeal laser surgery. The surgery does not require a neck incision as it takes place through the patient’s mouth. During surgery, we must balance widening the airway to improve breathing against risks of vocal breathiness and swallowing difficulty. Most patients achieve this balance. Usually they will have a breathy but functional voice, normal swallowing, and successful removal of the tracheostomy.
What we offer at Advanced ENT Centre
Dr Lau has a lot of experience treating vocal fold paralysis. He will make a thorough assessment and discuss your treatment options in detail.
He offers both video-stroboscopy and laryngeal electromyography for diagnosis.
Dr Lau pioneered minimally invasive injection for vocal fold paralysis in Singapore, introducing this to ENT practice in 2002. He continues to practice and refine the techniques, and teaches both locally and regionally on the subject.
He also performs open surgery for vocal fold paralysis and has trained in laryngeal reinnervation techniques.
In addition, Dr Lau has experience treating patients with paralysis of both vocal folds. He is experienced in micro-laryngeal laser surgery, and has achieved success de-cannulating patients with long-term tracheostomy for this condition.
How do I find out more?
Read more about services for throat, voice and swallowing disorders at Advanced ENT Centre.
Read more about conditions related to the throat, voice and swallowing.
Contact us at Advanced ENT Centre to arrange an appointment.