
What is thyroid surgery?
Thyroid surgery refers to the removal of part or all of the thyroid gland.
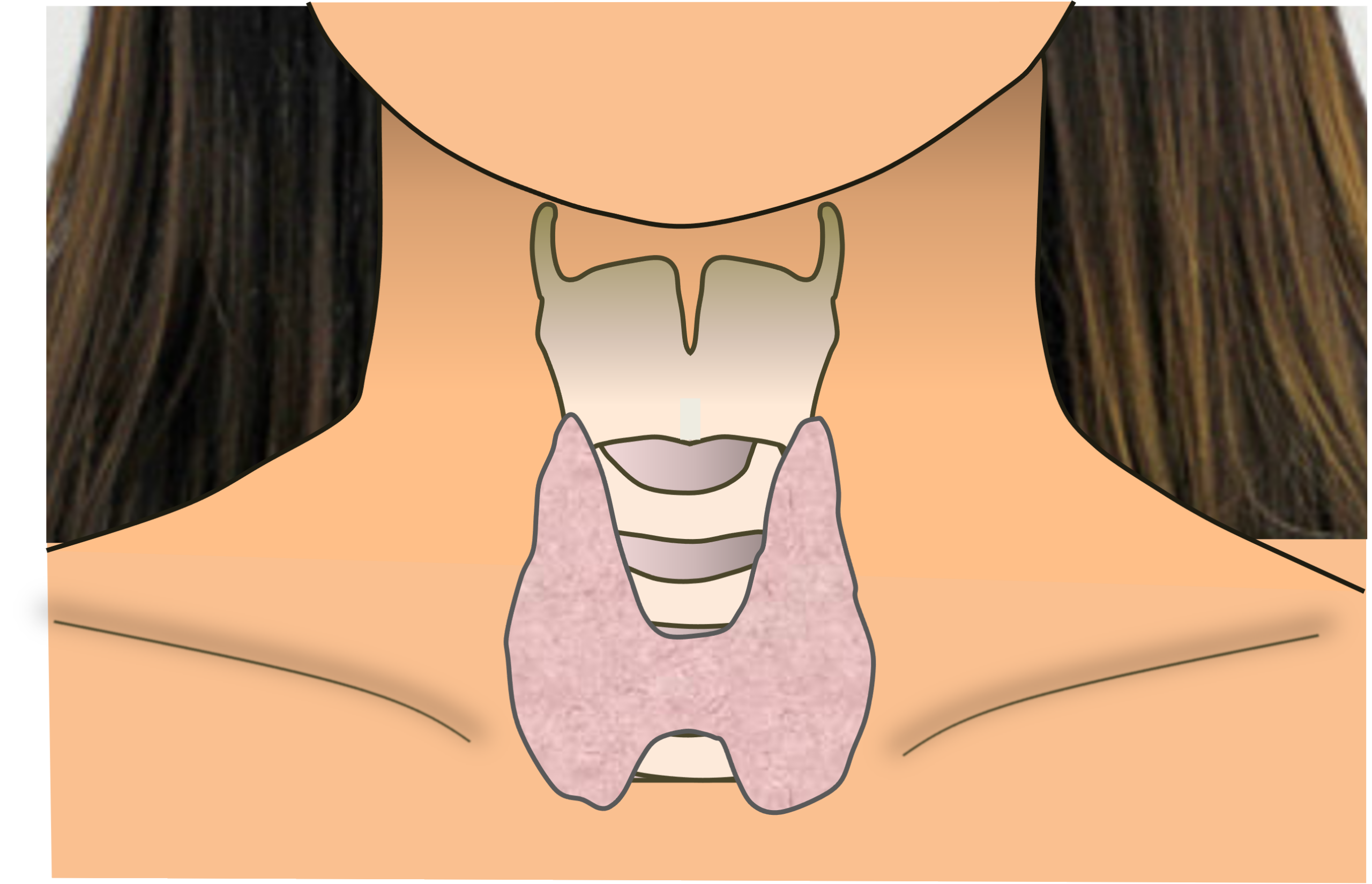
The thyroid gland is a butterfly-shaped organ that sits in front of the windpipe at the lower part of the neck. It secretes thyroid hormone, which controls your body’s metabolic rate, which roughly translated is the speed at which your body converts food to energy.
Why do I need thyroid surgery?
You may need surgery to remove a lump or nodule in your thyroid gland. Especially if there is concern that the lump could be malignant.
Other reasons for performing thyroid surgery are a nodule that is benign but causing discomfort in the neck. For instance, a large nodule can press on the food passage, causing swallowing discomfort, or compress the windpipe, causing difficulty breathing. Sometimes, an unsightly bump in the neck may be a reason to have it removed.
We sometimes perform surgery for autoimmune thyroid disease (Grave’s disease). This condition can make your thyroid gland overactive leading to problems in other parts of your body. Removing the gland can help overcome these problems.
Tell me more about the types of thyroid surgery
There are two main types of thyroid surgery: They involve removing either part of the gland or the whole gland. Removal of part of the gland usually means taking out half of the gland. We refer to this as partial thyroidectomy or thyroid lobectomy. We refer to removal of the whole thyroid gland as total thyroidectomy.
Do I need any tests before deciding on surgery?
You will usually need three tests before deciding on surgery.
Thyroid function test. This is a blood test to check if the thyroid is functioning normally or if it is over or under-active. An over- or underactive thyroid may need treatment with medication.
Ultrasound scan. This scan helps to characterize the nodule. In turn, characterizing the nodule helps us decide if we need to do a needle biopsy. Ultrasound is the most accurate way to image the thyroid gland, more so even than CT or MRI scans. This is good news because it is a simple, safe, and less expensive scanning method.
Fine needle aspiration for cytology (FNAC). FNAC allows us to extract cells from the nodule with a fine needle to determine the likelihood that the nodule is benign or malignant.
An ultrasound probe may help to guide the tip of the needle into the middle of the nodule. An on-site cyto-technician usually checks the biopsy sample immediately under a microscope to confirm if there are enough cells to make a diagnosis. We then send the sample to the lab where a pathologist makes the diagnosis.
The needle biopsy can tell us with a high level of accuracy if the nodule is benign or malignant. A benign nodule may not need surgery, whereas a malignant nodule almost always does. if uncertainty remains, we may have to repeat the biopsy, or recommend surgery if risk of malignancy is high.
What should I expect during thyroid sugery?
You will need to stay in hospital for three to five days, depending on whether you have a partial or total thyroidectomy.
The operation takes place using general anaesthesia, meaning that you are fully asleep. A breathing tube passed through the mouth into the windpipe allows the anaesthetist to control your breathing.
We usually make the surgical incision in the lower part of the neck. The incision measures about 5 centimetres. It typically falls just within the line of a crew neck t-shirt.
We usually use a special instrument called a harmonic scalpel to remove the gland. This uses ultrasonic vibrations to cut and cauterize tissue in a precise way that minimizes injury to adjacent tissue.
When surgery is complete, the nurses will monitor you in the recovery area of the operating theatre before returning you to the ward.
Back on the ward, we monitor how much blood drains from your neck through a small flexible tube known as a drain. The drain removes excess blood which would otherwise accumulate in the neck. When the drainage reduces, we can remove the drain and discharge you from the hospital.
Total thyroidectomy can cause calcium levels in the blood to fall. We measure this by checking calcium levels by a blood test after total thyroidectomy. If calcium levels are low you will need to start calcium replacement. We will need to ensure that the calcium levels are stable before discharging you from the hospital.
What should I expect after leaving hospital?
After leaving the hospital you must rest at home to recover from surgery. Subsequently, you must come back to the clinic after a week to have the suture removed. This is usually a single suture running in a zig-zag fashion just below the skin surface. Removing the suture is easy and painless.
We will also discuss your lab results at the follow-up visit. From here we can decide on the need for further treatment.
After total thyroidectomy, you will need to take thyroid hormone and calcium supplements. We need to monitor the calcium and thyroid hormone levels in your blood periodically.
What precautions should I take after thyroid surgery?
- Minimise touching the wound in the first 2 weeks after surgery. This prevents introducing infection which could affect healing.
- Keep the wound dry. Dry wounds heal better and are less prone to infection. We usually seal the skin with a special glue that forms a barrier to water and infection. Try to keep the wound dry during showering. If it becomes wet, you can use a hairdryer to dry it.
- Do not lift heavy objects until your wound has completely healed. This will prevent bleeding and swelling in the wound.
- Avoid stretching the wound. Examples of actions that stretch the wound are stretching the neck up, or twisting it. At the same time, it is important to maintain gentle mobility of your neck and shoulders to avoid these areas getting stiff.
What are the risks of thyroid surgery?
It is important to understand the risks of surgery and ask any questions you may have about them.
Risks common to both partial and total thyroidectomy
Anesthesia
Thyroid surgery requires general anesthesia meaning you are fully asleep. This is usually very safe. However you must inform the doctor of any medical conditions that you have and medication that you are taking. You may need a blood test and heart recording (ECG) to assess your fitness for anesthesia.
Wound complications
Most of the time, thyroid surgery wounds heal nicely. However, healing can vary between patients. In order to help your wound heal well and prevent infection, do follow the precautions from the preceding section.
Bleeding
Some bleeding into the wound is normal after thyroid surgery. However this gradually reduces over several days. Moreover the drain helps to prevent blood from accumulating in the neck. Severe bleeding can cause swelling in the neck and compression of the windpipe leading to difficulty breathing. This is rare but necessitates a visit back to the operating room to re-open the wound and stop the bleeding.
Hoarseness
There are three main reasons why hoarseness can occur after thyroid surgery.
Firstly and most important, is the risk of injury to the recurrent laryngeal nerve. This nerve runs just behind the thyroid gland and supplies the vocal folds. Injury to the nerve will paralyse the vocal fold. This results in a breathy or airy voice quality, and the voice is softer and harder to project. The nerve may recover, but if it doesn’t, we may recommend an injection laryngoplasty to strengthen the voice. Fortunately, the risk of injury is low (1-2%), but nonetheless, this is an important risk, particularly if you use your voice occupationally.
Secondly, hoarseness can arise from injury to the superior laryngeal nerve, which leads to a lowering of voice pitch. This is particularly important in females and in people who sing. We usually rehabilitate the voice in this situation using speech therapy, but surgery can help in severe situations.
Thirdly, and finally, hoarseness can also result from scarring of the tissues in the neck around the voice box. This is usually minor and recovers on its own.
Additional risks specific to total thyroidectomy (total gland removal)
Breathing difficulty
There is a small risk after total thyroidectomy of breathing difficulty due to injury to both recurrent laryngeal nerves (2%). This results in the vocal folds closing and blocking the windpipe entrance. The voice usually remains normal as the vocal folds come together.
If breathing difficulty is mild, we may simply wait to see if recovery occurs.
In the rare event that breathing difficulty is severe, we may need to create a small opening in front of the neck for a breathing tube called a tracheostomy to bypass the blockage at the vocal folds. We may need to perform a further operation to create a gap between the vocal folds to restore breathing. We usually perform this operation using microlaryngoscopy and a laser.
Low calcium levels in blood (hypocalcemia)
This may occur due to injury to the parathyoid glands. The parathyroid glands are four small glands, each about the size of a lentil, attached to the back of the thyroid gland. They are responsible for maintaining normal calcium levels in the blood. Without their function, calcium levels in the blood drop. We need calcium for normal muscle contraction, and low calcium can cause cramps and abnormal heart rhythm.
We overcome this problem by preserving at least one parathyroid gland. In addition, you will need to take calcium and vitamin D supplements until calcium levels are stable. The medical team will check your calcium levels shortly after surgery. If the levels are too low, we may need to replace calcium intravenously.
Low thyroid hormone level (hypothyroidism)
After a total thyroidectomy, we expect low thyroid hormone levels. Left untreated, this condition can cause severe lethargy and fatigue, among other problems. Fortunately, patients can easily restore thyroid hormone levels by taking thyroid hormone tablets daily. However, they must continue this treatment lifelong, and the doctor needs to perform periodic blood tests to check hormone levels.
Are there other considerations if I need total thyroidectomy for thyroid cancer?
There are several other considerations in thyroid cancer, including:
1. Lymph node dissection
Thyroid cancer sometimes spreads to the surrounding lymph nodes in the neck. The best way of detecting this is during an ultrasound scan. If the scan shows abnormal lymph nodes, we must clear these during surgery. We call this a therapeutic lymph node dissection. It usually involves the lymph nodes adjacent to the windpipe.
Sometimes, we need to perform lymph node dissection even if no abnormal lymph nodes appear on ultrasound. We refer to this as a prophylactic lymph node dissection and may recommend it if the tumour is large (>4 cm), has spread outside the gland, or if we discover large lymph nodes during surgery. The surgeon may clear lymph nodes from one or both sides of the windpipe.
2. Radioactive iodine treatment
You may need radioactive iodine treatment (RAI) following total thyroidectomy to “mop up” remaining thyroid tissue that could contain cancer cells. We usually recommend RAI for large tumours (>4cm), if the tumour has spread outside the thyroid gland, or if it has spread to the lymph nodes.
We usually administer RAI treatment orally, either by capsule or drink. The radioactive iodine seeks out thyroid tissue and destroys it with the radiation. Because most of the RAI collects in thyroid cells, the radiation affects the rest of your body less. Nevertheless, to prevent potentially exposing others to radiation, we will isolate you for a few days. Women should also avoid becoming pregnant for six months after treatment.
In order for thyroid cells to take up radioactive iodine, you need high levels of a hormone known as thyroid stimulating hormone (TSH) in the blood. We can achieve this either by witholding thyroid hormone replacement for 4 weeks (low levels of thyroid hormone signal the brain to produce more TSH), or by giving an injection of artificial TSH, known as thyrogen. The advantage of the thyrogen approach is that a person doesn’t have to stop taking their thyroid hormone supplements. Hence, they will not experience the adverse effects related to low thyroid hormone level.
3. TSH suppression
TSH suppression provides an additional safeguard against tumour recurrence. It works by using thyroid hormone tablets to signal to the brain to reduce the production of TSH. This may require an elevated dose of thyroid hormone to succeed.
High doses of thyroid hormone can cause adverse effects such as abnormal heart rhythm in older patients and increased risk of osteoporosis in postmenopausal women. Hence, we tailor the degree of TSH suppression according to the risk of recurrence. For example, when the risk of recurrence is high, we need greater TSH suppression (TSH <0.1 mU/L). However, if recurrence risk is low, then less TSH suppression is acceptable (TSH 0.5-2 mU/L). If the disease remains well controlled for five years, we typically maintain TSH between 0.5-2 mU/L, which is the low reference range.
We need to check thyroid hormone and TSH levels periodically to ensure that levels stay in the required range.
4. Monitoring for recurrence
We monitor for tumor recurrence by two methods:
1. Testing for a biochemical marker in the blood known as thyroglobulin, and
2. Checking the site of surgery for physical recurrences using ultrasound.
You will need to do these tests periodically, together with the blood test that checks thyroid hormone level and TSH suppression.
Are there alternatives to thyroid surgery?
Not all thyroid nodules require surgery, especially if they are benign (unlikely to be cancer, based on ultrasound and needle biopsy characteristics) and not causing symptoms. We usually follow up these nodules with ultrasound scans.
Taking medication such as thyroid hormone treatment is only useful if thyroid hormone levels are abnormal. We therefore do not use medication to treat most thyroid nodules.
We can treat fluid-containing nodules (cystic nodules) by aspirating the fluid from the cyst with a needle. Following aspiration, we can ablate the cyst by injecting it with alcohol.
We can also treat solid benign thyroid nodules that cause local symptoms with radiofrequency ablation. This treatment uses a radiofrequency needle probe to ablate the nodule under local anesthetic, and provides a minimally invasive alternative to surgery.
How do I find out more about thyroid surgery?
Contact us at Advanced ENT Centre to make an appointment to discuss your condition. Or read more about our services for neck lumps and thyroid.